"It doesn’t frighten me that Joe Biden is mentally unfit. What frightens
me is that millions know this and will still vote for him.”
— Robin Itzler
By Robin Itzler
Editor's Note: This is one of the commentaries selected from
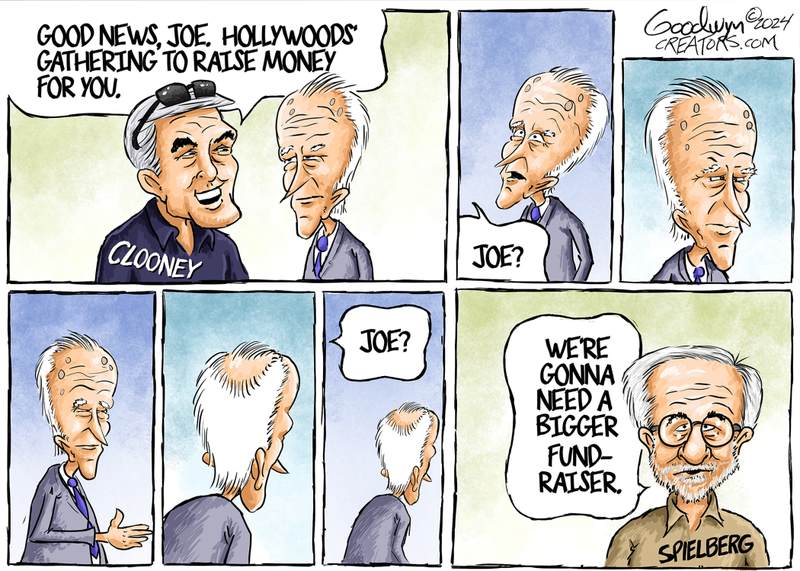
Robin's weekly newsletter Patriot Neighbors. Any cartoons appearing will
have been added by me. If you wish to get the full edition, E-mail
her at PatriotNeighbors@yahoo.com to get on her list, it's free. RK
On The DEMOCRAT Side:
Many are sulking off- and on-record that Joe Biden didn’t graciously step down (as once promised) and not seek re-election. From the embarrassing D-Day ceremony at Normandy to campaign speeches, Biden humiliates the United States with every utterance and movement. Speaking of movements, what president has ever been rumored to have them in public? Remember, our enemies read and see all this, too.
Hunter Biden was found guilty of all three felony gun charges. Now when Joey wants to call Trump a “convicted felon,” he can use the same adjective for his son who he has often said is the smartest person he knows. By the way, a person is only a “convicted” felon AFTER they have been sentenced by the judge. But be warned, this trial was a red herring! The Democrats purposely allowed the more crucial cases that would have shown Biden influence peddling to expire. Respected 538 pollster Nate Silver posted last week:
“But Biden just hit a new all-time low in approval (37.4%) at 538 yester-day. Dropping out would be a big risk. But there's some threshold below which continuing to run is a bigger risk. Are we there yet? I don't know. But it's more than fair to ask.”
On The REPUBLICAN Side:
From Karoline Leavitt, Trump Campaign National Press Secretary following the Hunter verdict:
“This trial has been nothing more than a distraction from the real crimes of the Biden Crime Family, which has raked in tens of millions of dollars from China, Russia, and Ukraine. Crooked Joe Biden’s reign over the Biden Family Criminal Empire is all coming to an end on November 5th, and never again will a Biden sell government access for personal profit.”
North Dakota held its primary on June 11 and passed "Congressional Age Limits” with nearly 61 percent of the vote. The new measure states that...:
"no person may be elected or appointed to serve a term or a portion of a term representing North Dakota in the U.S. Senate or the U.S. House of Representatives if that person could be 81 years old by December 31 of the year immediately preceding the end of the term, and any such person is prohibited from appearing on the ballot."
White
House Press Secretary Karine Jean-Pierre addressed the press Friday,
February 9, to highlight the work of the White House Office of Gun
Violence Prevention and the administration’s efforts in foreign
diplomacy. What she did not mention, however, was the lead story for
most media outlets in America that morning – the question of the
president’s cognitive health raised by the special counsel investigating
him over claims that he mishandled classified documents.
She did
turn over the podium to Ian Sams from the White House Office of Counsel
to the President. Sams addressed the report released by special counsel
Robert Hur Thursday by reiterating the point that no charges were
recommended and explaining that the president cooperated with an
extensive investigation. “The decision was that there was no case to be
made,” Sams declared before moving on to accuse Republicans of
fabricating a false narrative that there is a two-tier system in America
and that President Biden had been the beneficiary of special treatment.
(Photo by Nathan Howard/Getty Images)
The report
released Thursday by special counsel Hur exonerated President Biden of
any wrongdoing in the alleged mishandling of classified documents – but
it also brought up his age and apparently failing memory. In the report,
Hur characterized Biden as an “elderly man with a poor memory.” That
line sparked both a bevy of memes and multiple official responses by the
Biden administration – with Friday’s press briefing being the third in
less than 24 hours.
First, the White House published a letter
Thursday afternoon criticizing the special counsel’s characterization of
the president’s cognitive state and asking for a revision to the
report. Then the president himself spoke in an impromptu event Thursday evening to declare his memory sound.
Sams
did work his way around to attacking the sections of the report that
“gratuitously” commented on the president’s cognitive ability, though he
didn’t make the mistake of dwelling on the topic. Once reporters were
allowed to ask questions, however, the president’s mental state, the
validity of the report’s conclusion that Biden wasn’t guilty of anything
criminal, and the apparent disparity between what Sams calls the
“obvious” and correct conclusion and the allegedly “gratuitous” and
“politically motivated” parts of the report leading up to it. Sams
managed the worst of the questions with the skill of a master of spin.
Before ending the briefing, however, Jean-Pierre took the podium back
and tried to explain away and downplay the concerns over Biden’s
performance.
The implications
of the report’s claim about Biden’s cognitive state do not bode well,
however, for his re-election campaign or his desired image as a capable
leader. After a mishandled answer to one reporter’s question about
Israel, in which Biden mixed up Mexico and Egypt, the internet responded
with a flurry of new memes, such as a map of the region with Mexico in
place of Egypt and a picture of the Sphinx wearing a sombrero.
With
the report’s damning description and the president’s unfortunate gaffe
following the declaration that his memory is just fine – and, really,
his general performance during the late-evening speech – Biden’s
opponents certainly have fodder for their own campaigns. Can the White
House answer questions about the president’s mental health in a way that
solves the crisis, or will further attempts by the administration only
continue to make matters worse? Perhaps the far more important question,
will Biden remain defiant to the claims of cognitive decline, or will
he eventually bow out of the 2024 contest?
The World Health Organization (WHO) has admitted
that the very lockdown policies it advocated for have been instrumental
in a drastic increase in mental health issues on a global scale. In a report
published on Friday, the World Health Organization claimed that anxiety
and depression rose globally by a staggering 25 per cent in the first
year of Chinese coronavirus lockdowns, alone. As a result, the report
estimated that over one billion people worldwide are now suffering from
mental health issues.
“Restrictions imposed during the COVID-19 pandemic for example had
significant mental health consequences for many, including stress,
anxiety or depression stemming from social isolation, disconnectedness
and uncertainty about the future,” the W.H.O. stated.
The W.H.O. not only was instrumental in spreading Communist Chinese propaganda
about the ability of the coronavirus to spread from human to human but
was also a keen supporter of lockdown policies in response to the virus,
which were inspired by Beijing’s draconian reaction to the Wuhan virus..........To Read More.....
The story of American deinstitutionalization has become familiar. In a
long arc—from President Kennedy’s Community Mental Health Act of 1963
to the present—federal and state governments dismantled mental asylums
and released the psychiatrically disturbed into the world. Though there
were sometimes brutal abuses in the state mental hospitals of the early
twentieth century, the closure of the asylums did not put an end to
mental illness. If anything, with the proliferation on the streets of
psychosis-inducing drugs such as methamphetamine, the United States has
more cases of serious mental illness than ever before—and less capacity
to treat and manage them.
The question now is not, “What happened to the asylums?” but “What
replaced them?” Following the mass closure of state hospitals and the
establishment of a legal regime that dramatically restricted involuntary
commitments, we have created an “invisible asylum” composed of three
primary institutions: the street, the jail, and the emergency room. In
slaying the old monster of the state asylums, we created a new monster
in its shadow: one that maintains the appearance of freedom but condemns
a large population of the mentally ill to a life of misery.
I’ve spent the better part of two years looking at this invisible
asylum in West Coast cities. In major metropolitan areas such as Los
Angeles, San Francisco, and Seattle, the scale of mass psychosis is
overwhelming, and the inadequacy of the public response is self-evident.
It’s difficult, if not impossible, to imagine how public officials
could “solve” the problem of mental illness in these places, which are
home to tens of thousands of individuals suffering from the “perilous
trifecta” of mental illness, addiction, and homelessness. By contrast,
the contours of the problem are much more intelligible, even manageable,
in smaller cities and towns.
Olympia, Washington—a city of 52,000 tucked between a joint military
base and a state forest—is one such place. In Olympia, approximately 250
individuals have become entangled within this broken system of care,
cycling through the streets, the local jails, and the emergency ward at
Providence St. Peter Hospital. A half-century ago, many, if not most, of
these wayward souls would have been institutionalized. In 1962,
Washington State had
7,641 state hospital beds for a total population of 2.9 million; today,
it has 1,123 state hospital beds for a population of 7.6 million—a 94
percent per-capita reduction.
In the absence of the old asylums, Olympia’s mentally ill are now
crowded into a city-sanctioned tent encampment, then shuffled through
the institutions of the modern social-scientific state: the jail cell,
the short-term psychiatric bed, the case-management appointment, the
feeding line, and the needle dispensary. In the name of compassion, we
have built a system that may be even crueler than what came before.
It’s 8 AM, and
the streets of Olympia are at low tide. After months of coronavirus
lockdowns, all the businesses in the downtown core have shut down, with
some restaurants, salons, and tattoo shops boarding up their windows
altogether. The only people remaining are those with nowhere to go: the
homeless, the mad, and the addicted.
Patrol Sergeant Amy King and Officer Patrick Hutnik, who oversee the
downtown area for the Olympia Police Department, take me on a tour. The
officers are working their morning rounds, rousting awake people
sleeping in doorways and asking them to move on. We see a slumped-over
man who has soiled himself overnight, a man wrapped in cardboard
complaining that his tent got stolen, and three women behind a barricade
of shopping carts and filthy blankets. One of the women is tying off
her arm with a blue rubber strap but loosens her grip when she sees us;
the other two are barely cognizant, blinking at the officers and
lifelessly nodding their heads.
The cast of characters in Sergeant King’s world is a difficult one.
Hai air-fights through the streets because he believes monsters in the
ground want to enter his body. Michael, an old man, calls 911 many times
per day but doesn’t qualify as “gravely disabled.” Suburban Gary lives
in a broken-down Chevy Suburban full of trash but refuses all offers of
housing or services. And John, wheelchair-bound and covered in sores,
huffs paint in front of officers because he knows he’s “untouchable”—the
hospital will not take him, the prosecutor will not move on his
criminal cases, and the psychiatrists cannot send him for involuntary
treatment.
Following the downfall of the old regime of state asylums, local
jurisdictions have had to create their own makeshift mental-health
systems. In Olympia, as a growing population of mentally ill and
addicted individuals began to overwhelm downtown, the city council
decided to open the “mitigation site,” a publicly funded tent encampment
for 150 residents. In theory, the site would provide centralized
shelter and access to services; in practice, it functions as an open-air
asylum—with none of the protections of the old hospitals.
Brandon, who helps manage the mitigation site for the City of
Olympia, tells me that the people arriving here are “in the gutter.” He
estimates that 95 percent have a substance-abuse disorder and nearly 100
percent have a mental-health condition. Though the city continues to
distribute glossy photos from the site’s opening day, the reality on the
ground is grim—open drug use, fighting, crime, and even a tent filled
with used needles. Brandon says that “thousands of rats” have tunneled
under the site and will chew through the wooden pallets beneath the
tents and the plastic walls of the tiny homes. “There’s soy in the
plastic,” he explains. “It’s like candy to rats.”
“The city’s police force has nicknamed the mitigation site ‘The Thunderdome,’ after the Mad Max movie.”
By ordinance, the city provides mitigation-site residents with basic
social services and some access to care. Sean, a resident recently
released from prison in Idaho, landed at the site and got a prescription
for bipolar disorder “on the spot.” He shows me a plastic freezer bag
filled with bottles of carbamazepine and duloxetine, and explains his
predicament: “I found out, after 40 years, that I was bipolar. I lost
relationships, job, marriage. Now I’m trying to put everything back
together.”
But for most other residents, there is no treatment or recovery—only
the punishing routine of the needle, the pill, and the breakdown. The
city’s police force has nicknamed the mitigation site “The Thunderdome,”
after the dystopian Mad Max movie, because of the raucous
nights, with residents yelling, overdosing, and assaulting one another.
One former resident said that her boyfriend kept her imprisoned in a
tent there, plied her with methamphetamine, and put a knife to her
throat when she tried to leave—all under the supposed supervision of
city officials.
As they finish their morning rounds and head back to the station,
Sergeant King and Officer Hutnik find a disheveled, shirtless man,
passed out with his body extending into the street. Officer Hutnik
politely wakes him, and the man, known as Angry Marty, begins screaming
about zombies and food lines down at the mission. He manically gathers
metal piping tubes from the ground and bangs them into a shopping cart.
“There is going to be a mob that finally takes over this city!” he
screams. “They’re going to kill you! They’re going to kill you!”
Under the current policy regime, this madness has become an eternal
recurrence: the officers will see Marty again tomorrow morning, as he
suffers through another drug-terror, and they must leave him to fend for
himself.
As we head back to the station, we can still hear Marty’s cries in the distance.
“Is that compassion?” Sergeant King asks, disappearing into the doorway.
The Olympia Municipal Jail is the second
link in the city’s invisible asylum. It’s a small, doughnut-shaped
building tucked behind a Japanese garden, with white and blue stucco
walls. The jail has 36 beds, but the city generally won’t hold more than
28 inmates at a time because the old HVAC system can’t handle full
capacity.
After checking in at the front desk, Officers Holmes and Esselstrom
take me through the facility. They show me the intake desk, the
single-stall shower, and the suicide-watch room. They lead me through
the narrow hallways and flip open the steel viewing windows, so I can
see the men and women inside the cells.
I ask the officers how many of the inmates suffer from mental
illness. Officer Esselstrom says that they conduct an intake interview
for every inmate and that “at least 90 percent” say that they have been
diagnosed with a mental illness or have recently received psychiatric
care. The officers explain that they see the same faces, over and over,
often for the same crimes. “Some people have 40 different booking
photos,” says Officer Holmes, explaining that the officers sometimes
play a game in which they listen to the police radio and try to predict
who will come to the jail based on the nature of the call, crime, and
location.
Hannah is one of the inmates who has returned frequently over the
past year. She walks up to the metal visitation grate with some
hesitation, but after she learns that I’m not a representative of the
courts, she tells me her story in a rapid-fire monologue. Hannah grew up
in Auburn, California, and says that she was abandoned by her parents,
and then abused by her grandmother. She was diagnosed with ADHD as a
preteen, and after a series of fights and “explosive behavior” in high
school, she was re-diagnosed as bipolar. She says she got pregnant at
17, then lost the baby when she rolled her car and the seatbelt crushed
her stomach—which sent her life into a spiral. Over the next four years,
she started using methamphetamine, checked in and out of psychiatric
facilities, and then came to Olympia “to start over.”
That plan fell apart, too. For the past year, Hannah has lived on the
streets and at the mitigation site with her boyfriend, a man twice her
age and “a drug dealer and a pimp.” According to Hannah, they have been
involved in a long-running domestic dispute—knives, choking, biting,
drugs—and, despite mutual restraining orders, she always goes back to
him because “it’s hard to say no when he shoves meth in my face.” Today,
she has dirty hair and cracked skin, but it’s easy to see that she was
once beautiful. Officers told me that her mother once came looking for
her and brought an old high school portrait of Hannah with long hair and
intricate makeup—but when the mother eventually found the daughter on
the streets, she told everyone that Hannah was her boyfriend’s
responsibility and promptly left town. Now Hannah is stuck on the
streets and, when her methamphetamine addiction and bipolar disorder
manifest as violence, she ends up in the city jail.
Such stories are commonplace. Across the United States, the jails
have become de facto psychiatric hospitals. Bruce Gage, lead
psychiatrist for the Washington State Department of Corrections, estimates
that 20 percent to 30 percent of state prison inmates suffer from
serious mental illness. The Monroe Correctional Complex outside Seattle,
with nearly 500 beds for the mentally ill, is now the second-largest
psychiatric facility statewide; only Western State Hospital is larger.
“It used to be called deinstitutionalization,” Gage recently told the Seattle Times.
“Now it’s called trans-institutionalization. We took everyone out of
the state hospitals, and they pretty much, the same population, ended up
in prisons and jails.”
This transition from asylum to prison has reached an astonishing scale. According to a study
of 18,000 inmates in the Washington State prison system, 44 percent of
inmates were determined to have mental-health disorders and 51 percent
to have substance-abuse disorders—and 31 percent had both diagnoses
simultaneously. Even the old flagship, Western State Hospital, has
become a predominantly carceral environment, planning to accept only
“forensic patients” who can no longer be held safely in state prisons.
The irony is devastating: as a society, we recoiled from the old
asylums, but we have built in their place a parallel system that serves
the same function, often under even more brutal conditions. We have
adopted a new moral logic that says, “You have the right to be mad, but
if you follow that madness to its logical conclusion, there is a prison
cell waiting for you.” Under the weight of a cultural revolution against
the asylums and civil rights lawsuits against involuntary commitment, a
prison sentence has become the easiest option. The mentally ill get
subsumed into the criminal class.
The final link in the invisible asylum is
the psychiatric emergency room. In Olympia, this means Providence St.
Peter Hospital, home to an 18-bed psychiatric unit that functions as the
first stop for people coming off the streets in crisis. According to
Sue Beall, the hospital’s director of behavioral health, the emergency
psychiatric department receives approximately 500 people a month
presenting symptoms of acute mental illness and substance-abuse
disorders.
Beall describes the hospital as “overwhelmed.” The number of patients
seeking emergency psychiatric care has risen rapidly in the past few
years, and the hospital frequently operates beyond its regular capacity,
issuing “single bed certifications” and allowing people to rest on cots
in the hallways and mats on the floor. The severity of the cases has
increased, too. Beall estimates that, as recently as a few years ago,
only 20 percent of patients needed inpatient treatment; now that figure
is between 50 percent and 60 percent. The result: doctors, nurses, and
support staff are “spread too thin” and burning out under the pressure
of the city’s “revolving door” of addiction, psychosis, and emergency
care. Emergency rooms throughout the region are so pressed with mentally
ill patients that doctors have adopted a policy of “treat ’em and
street ’em”—that is, get patients medically stabilized and out as fast
as possible, to prepare for the next onslaught.
To reduce the burden on emergency providers, the City of Olympia
recently hired a Crisis Response Unit to patrol the streets and build
relationships with the most seriously mentally ill. The team—six men and
women in matching aqua-blue shirts—is headquartered in an open loft
space on the second floor of a downtown storefront. According to program
coordinator Anne Larsen, the Crisis Response Unit engages in more than
250 contacts a month, offering case management, referrals to services,
and even transportation to medical appointments. Yet despite some
successes—a woman placed into permanent housing, another living with her
sister on the Eastside—the team spends most of its time managing a
population of a few hundred mentally ill and addicted people who
continually cycle through their care.
To
reduce the burden on emergency providers, the City of Olympia recently
hired a Crisis Response Unit to patrol the streets and build
relationships with the most seriously mentally ill. (STEVE BLOOM/THE
OLYMPIAN)
When I arrive in the Crisis Response Unit’s offices, the team is
gathered around an old laptop and problem-solving some of their most
difficult cases. They’re talking through the file for Eddie, who was
living with his mother in rural Pacific County until she couldn’t handle
his mental illness, packed him up in an Airstream trailer, and dropped
him off on the streets of Olympia. Eddie began hoarding trash in his
trailer, increased his drug use, and rapidly deteriorated. Eddie’s
sister recently came looking for him and, together with the crisis
response team, tracked him down on the streets. They’re trying to
petition the court for a Joel’s Law detention—a form of involuntary
commitment for drug psychoses—but they have hit a bureaucratic
roadblock.
According to the crisis workers, it’s very hard to get any kind of
involuntary detention. Larsen says that the Crisis Response Unit
requests only one psychiatric hold evaluation per month, on average,
because the standard is so high and varies so widely from doctor to
doctor. The people on the streets, most of whom have gone through
repeated evaluations, have rehearsed the answers that will get them
immediately released: “I’m not a danger to myself or others, I know
where I can sleep, I know where I can get food.” When I ask the team how
difficult it is to get a long-term involuntary commitment at Western
State Hospital, their response is unanimous: “Impossible.”
In total, according to the latest available data,
designated crisis responders filed 1,599 petitions for involuntary
holds in Thurston County, and the courts approved only 411 cases for
inpatient detention—and the vast majority
of these were for short-term, 14-day holds. To illustrate how
challenging it is to secure an involuntary commitment, crisis workers
told me that they once found a woman eating a dead rat in an alleyway,
but this did not qualify her as “gravely disabled”; the reaction from
relevant officials was that “at least she’s eating.”
The mentally ill end up playing a game of cat and mouse with the
authorities. Jeremiah, a 32-year-old man in recovery from bipolar
disorder and alcohol and methamphetamine addiction, told me that he
would run wild in the streets: “I would be screaming at traffic, jumping
up and down on cars, yelling and cussing at families, saying their kids
are my kids.” At the end of one vodka-fueled bender, Jeremiah passed
out on the train tracks and lost both his arms to the heavy steel of a
freight locomotive. Even after his accident, the police department and
crisis response team spent years trying to get Jeremiah help, following
him through a series of short-term emergency visits, psychiatric
evaluations, and stints in the municipal jail.
Finally, something changed. Larsen, the program coordinator, pulled
every lever at her disposal and organized the entire apparatus of local
government to pressure Jeremiah into accepting treatment. It took a
massive mobilization—involving a hospital ward, an evaluation center, a
jail term, two treatment programs, a halfway house, a street
intervention, and a warrant hearing—but eventually Jeremiah relented. I
asked him what had changed, and he said: “I called my mom on Mother’s
Day from jail. I wanted to do something with my life.”
Jeremiah now stays at a recovery home on the edge of town. When I
visit him there, he says that he has been sober for more than a year.
“It’s my longest time clean since I was 11 years old,” he says. Jeremiah
still distrusts authorities—when I took out my notebook, he asked if I
was trying to get him recommitted—but acknowledges that he wouldn’t have
gotten clean without the intense pressure of the local government.
“Treatment was necessary,” he says, “even if I didn’t like how it came
to me.”
In 1961, French theorist Michel Foucault reenvisioned the history of mental illness in his book Madness and Civilization,
which documented the role of confinement, morality, and medicine from
the Middle Ages to modernity. Foucault yielded some profound insights,
but, like his radical-progressive American counterparts, he savaged the
practice of confinement without proposing a substantive alternative.
Nearly 60 years later, it has become clear that the liberationists of
the 1960s did not usher in a new era of freedom but something far
darker. By reducing the entire cultural history of madness to one long
progression of brutality, imprisonment, and false care, they laid the
political groundwork for deinstitutionalization. At the same time, their
insistence that mental illness was a “myth,” that it could be cured by
new psychiatric drugs, or that it would be transformed through political
consciousness turned out to be wrong.
Today, a consensus is emerging that deinstitutionalization went too
far. In Washington State, a bipartisan coalition of legislators has
implemented the beginnings of a reform agenda. In the past few years,
the legislature has added acute substance-abuse disorder as a condition for involuntary treatment, extended the initial involuntary hold period from 72 hours to five days, and adopted plans to add 844 new inpatient psychiatric beds across the state. The state mental-health budget has nearly doubled in recent years, with widespread support from both Democratic and Republican lawmakers.
Do these reforms go far enough? Probably not. Washington hopes to increase
its psychiatric bed capacity to 1,763 beds by 2025, or 23 beds per
100,000 residents. While that’s a significant increase from the current
baseline, the goal still falls far short of the historical average of
263 beds per 100,000 at the height of the asylum period. Though advances
in psychiatric drugs and outpatient treatment could reduce the total
need for inpatient beds, it’s illusory to believe that we can operate at
9 percent of the capacity of the 1960s. For anyone who has witnessed
the great masses of the mad wandering the streets of American downtowns,
it’s obvious that our cultural and legal intransigence against
confinement cannot hold.
Frontline workers in the current system understand this reality but
hesitate to offer their full-throated endorsement of rebuilding the
hospitals. When I ask Sergeant King for her opinion on the need for more
involuntary psychiatric beds, she replies cautiously. “I have to be
careful. I don’t want my words twisted,” she says, calibrating her
language in order to avoid the charge of “criminalizing” mental illness.
“I think we were too restrictive in the past, but we’ve swung the
pendulum too far in the other direction.”
Perhaps what’s most needed is a renewed theoretical defense of the
principles of the asylum—safety, rest, morality, and health—that
Foucault and his compatriots demolished. This does not mean a return to
the historical practices of the asylum but a revival of the spirit that
animated the care and moral reasoning of the old retreats and hôpitaux. It is a moral scandal that our society, which has surpassed
the material wealth of the nineteenth century 16-fold, cannot provide
an adequate sanctuary for the mad and the unmoored. It’s easy to condemn
the horrors of the old state hospitals, but the horrors of the
invisible asylum may exceed them.
“Perhaps what’s most needed is a renewed defense of the principles of the asylum—safety, rest, morality, and health.”
In my short time on Olympia’s streets, I
heard about a litany of abuses and indignities that occurred under our
current regime—a disabled man whose feet are rotting off, a woman hunted
down like prey, a woman waking up on top of a corpse.
But the neglect is even more heartbreaking. Whenever I consider
today’s system, I see the awful silhouette of a young man crumpled
across a restaurant ingress, bare-chested and overwhelmed with madness.
He introduces himself as Harrison and, revealing a Hindu-style third eye
tattooed on his forehead, rattles on about angels and demons. He points
to Officer Hutnik and says: “I once cured you of an infection.” Then he
picks up an old Rubik’s Cube from his pile and, twitching with feverish
intensity, points to the white squares and says, “This is where you can
find me anywhere in the universe.”
A more muscular system of care could help this haunted soul. After we
say good-bye to him, Hutnik tells me that he remembers Harrison from
his time as a correctional worker at the Thurston County Jail a decade
ago. “It’s amazing how you see another side of people after they’ve
detoxed and gone on medication in jail,” Hutnik says. And this is
precisely the insanity of our current system: in fear of “criminalizing
mental illness,” we have simply delayed care until the mentally ill
engage in explicit criminality. We thus condemn legions of vulnerable
people like Harrison to street, jail, or emergency room. Until we
rebuild the physical capacity and moral strength to help them, nothing
will change.
Christopher F. Rufo is a contributing editor of City Journal
and director of the Discovery Institute’s Center on Wealth &
Poverty. He has directed four documentaries for PBS, including his new
film, America Lost.
Top Photo: An outreach worker arrives under Olympia’s Fourth
Avenue Bridge to assist homeless people residing there. (KEN LAMBERT/THE
SEATTLE TIMES)
City Journal is a
publication of the Manhattan Institute for Policy Research (MI), a
leading free-market think tank. Are you interested in supporting the
magazine? As a 501(c)(3) nonprofit, donations in support of MI and City Journal are fully tax-deductible as provided by law (EIN #13-2912529).SUPPORT
Have mercy...on those infected with MRSA
This HND piece covers yet another outbreak of methicillin-resistant Staphylococcus aureus aka MRSA. What makes this one plain awful is that it occurred in a neonatal intensive care unit, and would not have even been reported publicly, but for "leak" from a hospital employee to a state official. You'll love the excuse they used when confronted by the media. My friend, infection control guru Lawrence Muscarella, weighs in on this, and while polite, he minces no words. Read the complete article.
This HND piece discusses how retired and suffering NFL players are turning to cannabidiol (CBD) to relieve their symptoms. Unlike denial, which was the NFL's primary response to concussions, the league sure knows how to deal with chronic pain—and that's with drugs. Loads of them. Too bad there are side effects. Way back in the 60s, I knew a UCLA football player (a defensive back) who was taking enormous doses of ibuprofen for his constant pain. While I guess it helped him with the pain, it also burned out his kidneys. Too bad they didn't have CBD back then. One of the groups promoting CBD to the former players is CW Hemp, famous for coming up with the formula that saved the life of little seizure sufferer Charlotte Figi. (CW as in Charlotte's Web). CBD is a cannabis extract that has no hallucinogenic properties, but does wonders for a variety of symptoms. Naturally, the Feds are years behind the curve on this one. Read the complete article.
This HND piece examines the very real problem of prescription drug abuse. The title derives from the sad fact that a majority of abused prescription drugs are obtained from family and friends, including from the home medicine cabinet. We cite some disturbing statistics, including this charmer: 45 people die every day from overdosing on opioid prescription painkillers, and that's more deaths than fatal heroin and cocaine overdoses combined. The good news is that the government and private sector are teaming up in a big way to mbat this epidemic. Read the complete article.

")